A chalazion is one of the most common — and at the same time most misunderstood — eyelid problems.Many people:
- develop a chalazion
- treat it
- and a few months later… see it come back
and a few months later… see it come back
Sometimes:
- in the same eye
- other times in the other eye
- often in the exact same spot
And naturally they wonder:“Why does it keep coming back?”“Did I not treat it properly?”
The truth is that, in most cases, the chalazion is not addressed at its root cause.
What a chalazion really is
- is not an infection
- is not a “pimple”
- is not always caused by microbes
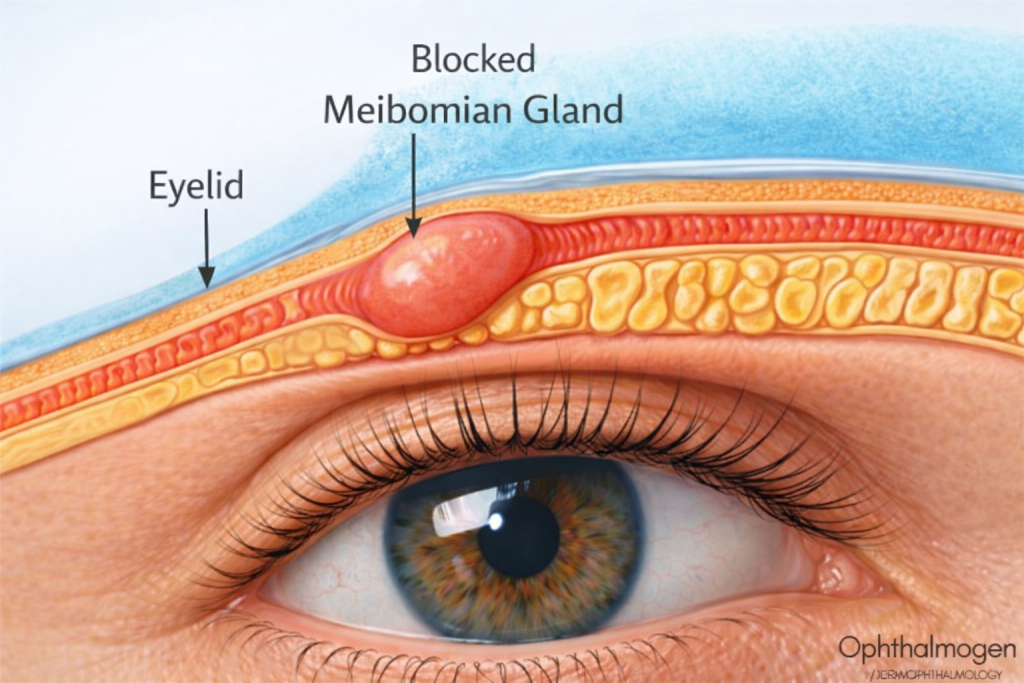
A chalazion is a blockage of a Meibomian gland in the eyelid.
Meibomian glands:
- are located within the eyelids
- produce the lipid (oily) layer of the tear film
- help tears “stay” on the eye
When their contents:
- become thicker
- stagnate
- stagnate
a chalazion forms.
Evidence note: The classic description of chalazion as Meibomian gland blockage/inflammation and first-line conservative management with warm compresses is described in clinical references/guidelines (e.g., StatPearls, NHS/NICE).
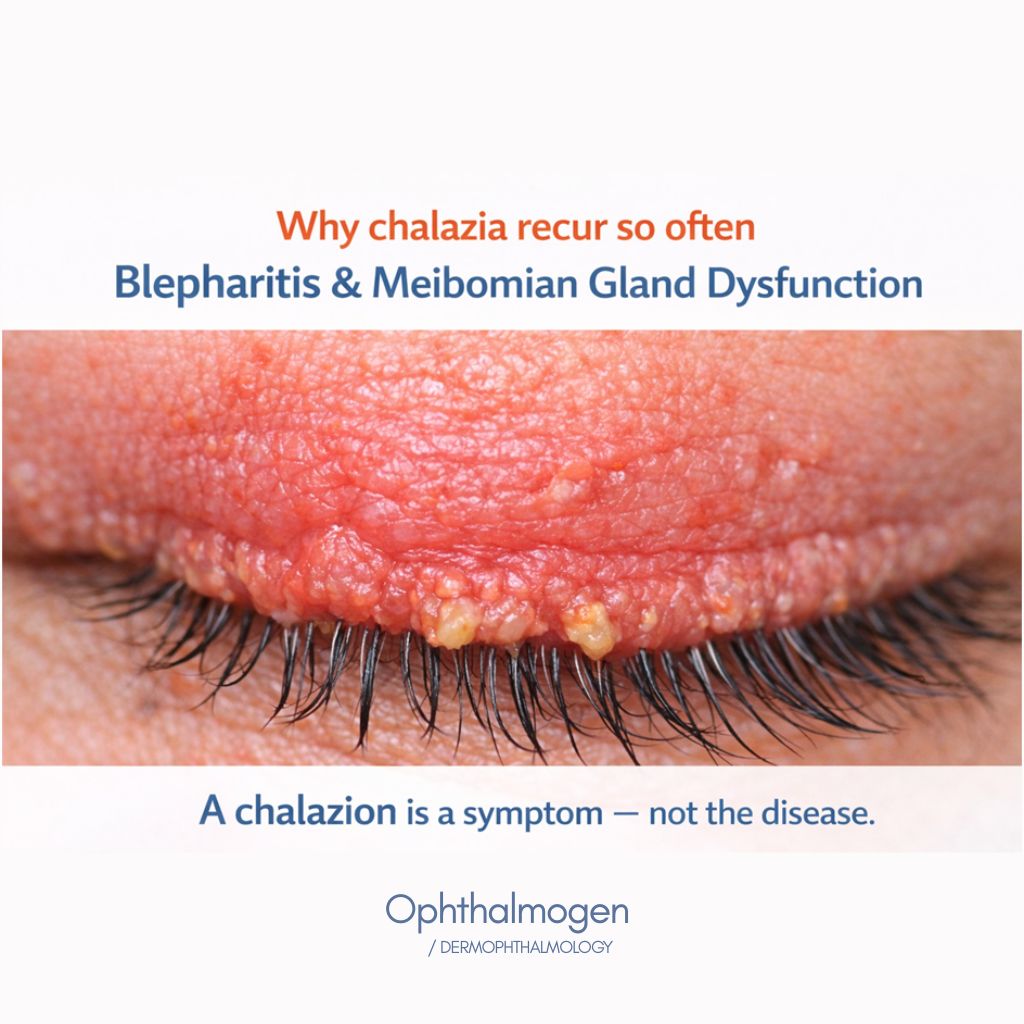
Why chalazia recur so often
This is the key point.In the vast majority of cases, chalazion is associated with:
- underlying blepharitis
- or Meibomian gland dysfunction (MGD)
If:
- eyelid hygiene is not restored
- meibum flow does not improve
- the eyelid “environment” doesn’t change
then the gland will block again. A chalazion is a symptom — not the disease.
Evidence note:MGD/blepharitis as a major driver of tear film instability and chronic ocular surface dysfunction is discussed extensively in TFOS DEWS II (2017).
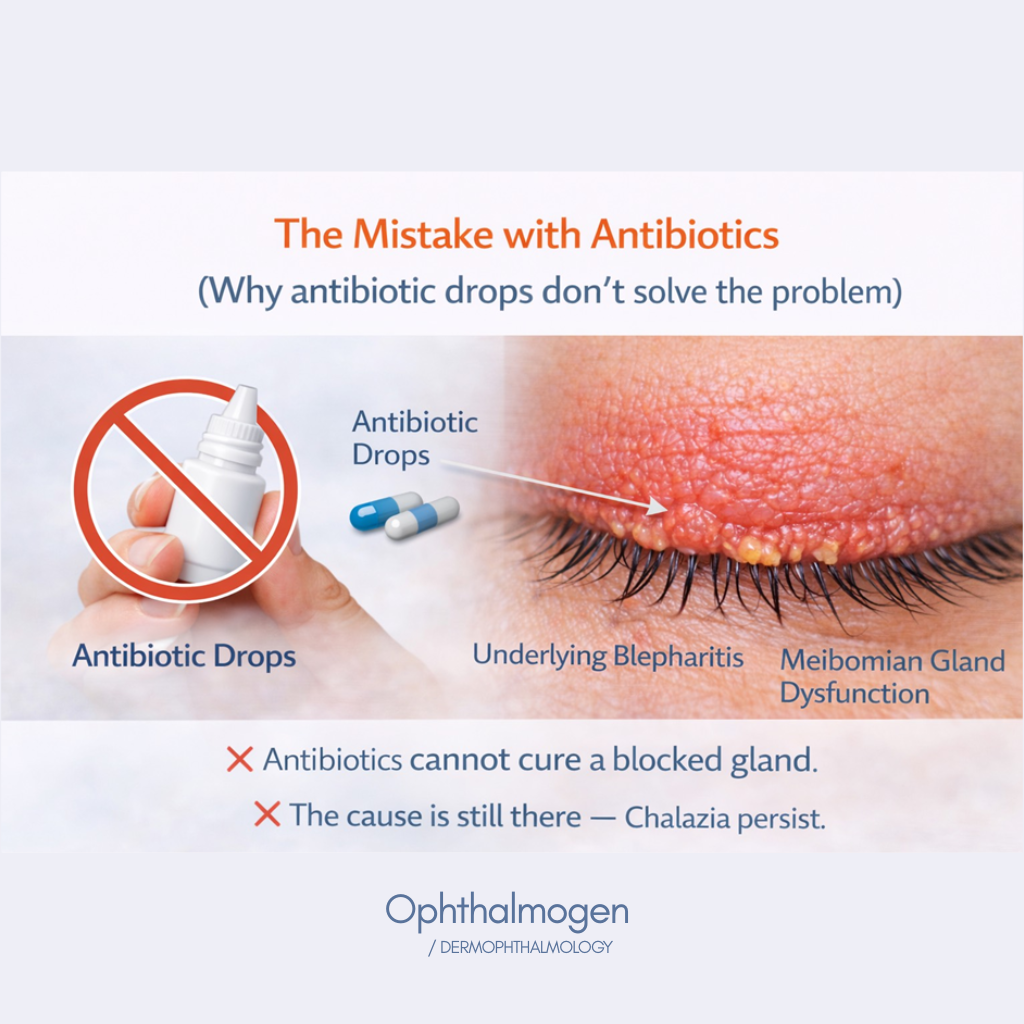
Why antibiotic drops often don’t solve the problem
Why antibiotic drops often don’t solve the problem
- Tobrex
- Tobradex
These medications:
- can be helpful when there is secondary infection
- can temporarily reduce inflammation
However
- they do not unblock glands
- they do not liquefy thick meibum
- they do not restore eyelid function
That’s why:
- the chalazion improves
- but then recurs.
Evidence note: In uncomplicated chalazion (not an infection), the core conservative approach is heat/hygiene; antibiotics are used when there is infection/superinfection or a clear indication.
The oral hygiene analogy (to make this crystal clear)
Think of it like this:
- A chalazion→ tooth decay (cavity)
- - blepharitis→ gingivitis
- Do Artificial tears→ mouthwash
- Eyelid hygiene → brushing & flossing
If you only use mouthwash but don’t brush your teeth,the problem returns.Exactly the same logic applies to eyelids.
The role of artificial tears (and their limits)
Artificial tears such as:
- Visionlux Plus Duo
- Navitae Plus
- THEALOZ Duo
- Systane
- Flora Vision Spray
are:
- necessary
- useful
- soothing
They help with:
- hydration
- diluting inflammatory factors
- improving comfort
But they do not address the cause of chalazion.
They do not:
- unblock glands
- restore lipid balance
- treat blepharitis
That’s why they should be complementary — not the only solution.
Evidence note:TFOS DEWS II distinguishes symptomatic relief (lubricants/artificial tears) from interventions that target MGD/lipid layer/eyelids
Chalazion as an eyelid problem (Dermophthalmology approach)
Modern thinking treats chalazion as:
- a skin-and-gland problem
- not simply an “eye problem”
This is the core of Dermophthalmology:The eyelid is the key.

The role of the Ophthalmogen line in chalazion (a natural approach — without drugs)
The Ophthalmogen products:
- is not pharmaceutical therapy
- is not an antibiotic
- is not steroid-based
And that’s exactly its advantage — especially in chronic, recurrent chalazion cases.
Ophthalmogen products:
- support normal Meibomian gland function
- improve meibum flow
- reduce conditions that promote blockage (e.g. Demodex)
- help both with improvement and — most importantly — prevention of recurrence
This is a natural, non-drug way to address the cause,not just the symptom.
Why this matters most in recurrent cases
In people who:
- develop chalazion again and again
- have blepharitis or MGD
- frequently use Tobrex / Tobradex
The problem is no longer “acute”, it’s chronic and functional. And chronic problems:
- are not solved with repeated medication cycles
- but with consistent support of the underlying mechanism.
Just like:
- you don’t take antibiotics for gingivitis every month
- you improve oral hygiene.
- Ophthalmogen products does not replace medication when it’s truly needed —but it’s the natural way to reduce the need for it again.
How to apply the prevention framework correctly
OphthalmogenEYE10 — Thermal decongestion
- 1–2 times per week
- liquefies thick meibum
- helps keep glands open
- reduces the chance of new blockage
Ophthalmogen products Gel — Eyelid massage
- gentle massage
- increases meibum mobility
- reduces micro-inflammation
- ideal after heat
Ophthalmogen Spray — Daily support
- use during the day, especially in front of screens
- increases blinking
- supports the natural flow of secretions
- easy to use anywhere
Naviblef Daily Care/ Ophthalmogen
- essential for people with a history of recurrent chalazia
- reduces blepharitis load
- cleans gland openings
This combination helps prevent recurrence..
Evidence note:Eyelid warming/heat therapy and eyelid hygiene are core pillars in MGD/evaporative dry eye management and are discussed in clinical literature and reviews (e.g., The Ocular Surface/TFOS, OPTO review, and studies assessing warm compresses/warming devices).
FAQ
Why does my chalazion keep coming back?
Why does my chalazion keep coming back?
Should I keep using antibiotics repeatedly?
Not if there is no infection.
Do Artificial tears help?
Yes — but they aren’t enough on their own.
Can it be prevented?
Yes. Just as you prevent tooth decay through hygiene actions, you can reduce chalazion recurrence with massage, spray support, and controlled warming.

In Summary
- A chalazion isn’t just “bad luck”
- It isn’t solved only with drops
- It isn’t always a microbe problem
- It’s an eyelid problem
- It needs prevention
- Proper hygiene changes the trajectory
Just as teeth need daily care,so do eyelids.
Brief scientific references (for the end of the article)
- TFOS DEWS II (2017), The Ocular Surface (staged management, MGD/evaporative dry eye, eyelid role).
- NHS/NICE & StatPearls: chalazion definition/management, warm compress role, antibiotic indications.
- Bzovey B. (2022), OPTO review: eyelid warming devices, clinical role, compliance/effectiveness of warming.
- Murakami DK et al. (2015): evidence on warm compress/eyelid warming effectiveness in MGD (abstract).